
I previously wrote an article on ChrisKresser.com called “Is Gluten Sensitivity Real” which critiqued a spate of news reports suggesting that nonceliac gluten sensitivity (NCGS) doesn’t exist. These news stories referred to a study indicating that some people who believed they were reacting to gluten were actually reacting to a class of poorly absorbed carbohydrates (which include wheat, among many other foods) called FODMAPs.
You can read the full article above for details, but the takeaway was that the study those stories were based on in no way disproved the existence of NCGS, nor did it overturn the large body of evidence that links it to a variety of health problems ranging from type 1 diabetes, to allergies, to schizophrenia, to autism spectrum disorders. There is little doubt among those who are familiar with the scientific literature that NCGS is a real condition.
Yet despite this, we continue to see headlines in the media like this:
- Time for Some Grains of Truth About Gluten
- Eat More Gluten: The Diet Fad Must Die
- Why We’re Wasting Billions on Gluten-Free Food
These stories—and many other like them—argue that nonceliac gluten intolerance is rare, and that people who eliminate gluten from their diet are just silly fad followers. In this article, however, I’m going to present three reasons why NCGS is not only a bonafide condition, but may in fact be a much more serious problem than celiac disease.
#1: Celiac disease is far easier to diagnose than NCGS
According to some estimates, for every diagnosed case of celiac disease (CD), there are 6.4 undiagnosed cases that remain undiagnosed—the majority of which are atypical or “silent” forms with no damage to the gut. (1) This silent form of CD is far from harmless; it is associated with a nearly fourfold increase in the risk of death. (2)
I believe that patients with NCGS are even more likely than patients with CD to go undiagnosed. Most gastroenterologists today know how to screen for celiac disease. They will typically test for antibodies to antibodies to alpha gliadin, transglutaminase-2, deamidated gliadin, and endomysium, and if positive do a biopsy to determine if tissue damage is present.
However, we now know that people can (and do) react to several other components of wheat above and beyond alpha gliadin, the component that is implicated in CD. These include other epitopes of gliadin (beta, gamma, omega), glutenin, wheat germ agglutinin (WGA), gluteomorphin, and deamidated gliadin. What’s more, people can react to other types of tissue transglutaminase, including type 3—primarily found in the skin—and type 6—primarily found in the brain. (3, 4, 5, 6, 7, 8)
Why the “gluten intolerance haters” are wrong.
So, imagine a scenario where the patient is reacting to deamidated gliadin, glutenin, gluteomorphin, and either transglutaminase-3 or -6, but not reacting to alpha gliadin or transglutaminase-2—which are the antibodies used to screen for CD by most doctors. They will remain undiagnosed, and may continue to eat gluten for the rest of their lives, putting themselves at serious risk for autoimmune and other diseases.
This is not a hypothetical situation. In fact, I see cases like this all the time in my practice. Here is a screenshot from a recent test I ran on a patient. I use a much more thorough test for wheat and gluten intolerance called Array 3 from Cyrex Laboratories. Unlike other tests, it measures antibodies not only to alpha gliadin and transglutaminase-2, but also many of the other components of the wheat protein I mentioned above, as well as transglutaminase-3 and 6.
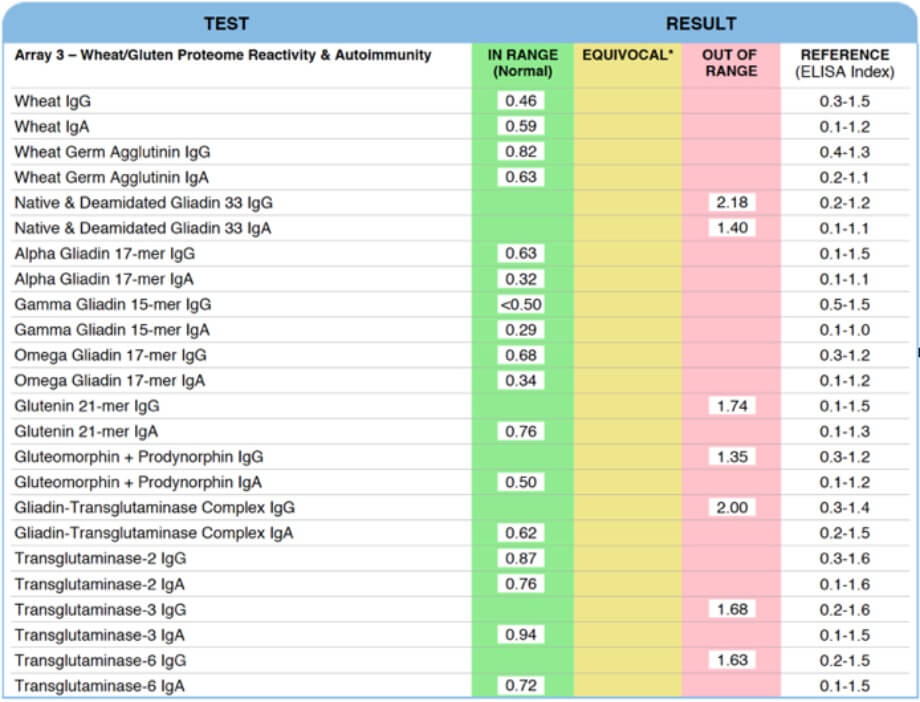
This patient is not reacting to alpha gliadin or transglutaminase-2. Had they been tested by their conventional doctor, they would have been told that they do not have celiac disease or gluten intolerance.
However, as you can see, she is reacting quite significantly to several different components of wheat, including:
- Native and deamidated gliadin and gluteomorphin, which are compounds produced during the digestion of wheat.
- Glutenin, which is the other major fraction of the wheat protein, along with gliadin.
- Gliadin-transglutaminase complex, which indicates that the patient is experiencing an autoimmune reaction to wheat.
- Transglutaminase-3, which is expressed primarily in the skin, and to a lesser extent in the brain and placenta.
- Transglutaminase-6, which is expressed in the brain and nervous system.
When this patient consumes wheat or other gluten-containing foods, she may not experience the classic digestive symptoms associated with CD or NCGS, because she is not producing antibodies to transglutaminase-2 (which is mostly expressed in the gut). Instead, her intolerance of wheat could manifest in skin conditions like eczema or psoriasis, and in neurological or brain-related conditions like depression, peripheral neuropathy, or ADHD. (9, 10)
Worst of all, if this patient had not had this test, and had continued to eat wheat and gluten for the rest of her life, it’s likely that she would have been at much higher risk for the long list of serious conditions that are associated with gluten intolerance, such as multiple sclerosis, ataxia, diabetes, and even Amyotrophic Lateral Sclerosis (Lou Gehrig’s disease). (11, 12, 13, 14)
Unfortunately, this patient is not the exception—she is the rule. I’ve seen so many test results just like this, where the patient would have been misdiagnosed as not having gluten intolerance had they gone to a conventional doctor.
This presents another obvious problem, of course: if very few health care providers are doing the correct testing for gluten intolerance (like the panel from Cyrex above), then how can we possibly know what the true prevalence of NCGS is? We can’t—but given everything I’ve written above, we can certainly suspect that it’s much higher than currently believed.
According to Cyrex Labs, 1 in 4 people that take the Array 3 panel test positive for some form of wheat or gluten intolerance. Granted, this is not a representative sample, since most people that take the Cyrex panel are dealing with chronic illness of some kind.
Even with the limitations of current testing, however, some researchers have speculated that NCGS may affect as many as 1 in 10 people. (15) I suspect this is accurate, if not conservative.
#2: Current cultural attitudes toward NCGS mean more people will remain undiagnosed
There has been a big backlash in both the mainstream media and on social media channels against the idea of gluten intolerance. Despite overwhelming evidence to the contrary, uninformed journalists and armchair Facebook scientists continue to argue that NCGS is some kind of widespread collective delusion—simply a figment of the imagination of anyone who claims to experience it. And for reasons that I do not fully understand, they do so with an almost religious fervor.
The “gluten intolerance haters” seemed to emerge in force after a paper published by Gibson et al. in 2013 made the rounds in the media. This study found that a group of patients with irritable bowel syndrome (IBS) were not sensitive to gluten, but instead were reacting to a group of poorly absorbed carbohydrates called FODMAPs. (16) Aside from the fact that this study did not in any way disprove the existence of NCGS, from a practical perspective the study findings would not have changed the behavior of most people with IBS who identified as being gluten intolerant, since wheat and many other gluten-containing grains are FODMAPs and should thus be avoided by these patients.
More importantly, however, in the last two years since the Gibson paper new studies have been published that directly contradict Gibson’s findings and strongly suggest that patients with IBS do, in fact, react adversely to gluten—and not just FODMAPs.
For example, a new double-blind, randomized trial out of Iran was specifically designed to determine whether a group of IBS patients reacted to gluten specifically, or simply improved for other reasons on a gluten-free diet. (17) Here’s how it worked:
- 80 patients followed an “almost-gluten-free” diet (dietary compliance was considered optimal if consumption of gluten was below 100 mg/day, the equivalent of roughly 1/8 tsp of wheat four).
- After six weeks, the 72 patients that complied with the diet and experienced significant improvement were then randomized into two groups: Group A, and Group B.
- Group A (35 patients) was given a 100 g packet containing a gluten meal (free of FODMAPs). Group B (37 patients) was given a placebo packet (100 g) containing rice flour, corn starch, and glucose.
- Patients in both groups consumed the powders for six weeks, while both groups continued on gluten-free diets.
After six weeks of the diet symptoms were controlled in only 26% of the gluten group, compared with 84% of the placebo group. In the gluten-containing group, all symptoms—especially bloating and abdominal pain—increased significantly one week after starting the gluten.
The authors point out that it is important to properly identify gluten intolerance and distinguish it from FODMAP intolerance because some recent research suggests that long-term low FODMAP diets may have adverse effects on the gut microbiome. One study found that a low FODMAP diet compared with a habitual diet reduced the proportion and concentration of Bifidobacteria, one of the most beneficial species of bacteria in the colon. (18) (Authors note: I will be exploring this issue in more detail in a future article.)
But I would add another equally serious consequence of misdiagnosing gluten intolerance as FODMAP intolerance, which is the increase in risk for numerous and sometimes serious diseases that occurs when someone with NCGS continues to consume gluten.
#3: Many doctors and patients aren’t serious enough about NCGS treatment
This last point is a natural consequence of the first two. If detecting NCGS in conventional medical settings is unlikely, and there is a strong cultural backlash against it, where does that leave the millions of people that are likely suffering from NCGS without even knowing it?
Even if they do suspect that they are gluten intolerant, they might be dissuaded from pursuing a strict gluten-free diet by their friends, social media contacts, or even their doctor, all of whom are likely uninformed on this subject and do not understand the deficiencies in conventional testing or the complexity of the topic.
Based on the research I’ve reviewed in this article, and several others I linked to here, we should be more aggressive—not less—in diagnosing and treating gluten intolerance.
We need greater access to test panels like Cyrex Labs Array 3, which is the only commercial test outside of a research setting that screens for antibodies to many of the proteomes in wheat, instead of just testing for alpha gliadin. We need better training for doctors on how to recognize the myriad of symptoms and conditions associated with gluten intolerance, so they don’t make the common mistake of assuming that the patient isn’t gluten intolerant if they don’t have digestive problems. And we need some prominent journalists to educate themselves, step forward, and take responsibility for treating this as the serious, potentially life-threatening problem that it is.
Even without access to tests like Array 3, an elimination/provocation trial where gluten is removed completely from the diet for 60 days and then reintroduced is still considered to be an accurate method of assessing gluten intolerance. Doctors should be much more proactive about recommending this to patients, and despite the claims of some mainstream nutritionists and dietitians to the contrary, there is no risk to removing gluten from the diet. (19) If anything, people on a gluten-free diet are more likely to increase their intake of essential nutrients, especially if they replace breads and other flour products with whole foods (rather than with gluten-free flour alternatives).
Finally, it’s worth pointing out that many people that are intolerant of gluten are also intolerant of other food proteins found in foods like dairy, eggs, and unfortunately, coffee. Studies have shown that about 50 percent of patients with CD show intolerance to casein, a protein in milk. (20)
This may explain why up to 30 percent of CD patients continue to have symptoms or clinical signs after adopting a gluten-free diet. (21) For this reason, I recommend a completely grain- and dairy-free diet during the gluten challenge period.



The denial of ncgs is reminiscent of the claim that EBV only caused kissing disease and then 20 yrs later they finally said that it could damage the spleen and pancreas, which can lead to decreased immunity and faulty food metabolism, and even a higher risk of certain cancers. Or how CFS was all in the mind, and now it has a real name and better treatments. And of course there’s the reminder that they used to think cancer was hysteria and people died of it in mental asylums. Seems the denial of ncgs may have to do with the decreased sale of gluten. Who knows, someone is always trying to tell sick people that they’re imagining things, even in 2017! Thanks for the great article, next they will say that wonderfully detailed lab test is meaningless. I would disagree, as it shows thorough knowledge more than most Dr’s have. Good luck.
My mother was diagnosed with ALS in May 2014. Her doctor put her on riluzole, letting her know there was no cure but the medication might provide her a few more months of delayed symptoms. ALS progresses at different rates and affects different body parts first. My mother, being 73 at the time, fell into a category of what they call “fast progression” (older female). Her arms weakened first, then her hands, her mouth, and throat, and finally her lungs. Throughout her two-and-a-half-year ordeal, she was able to walk with assistance nothing was really working to help her condition.I took her off the riluzole (with the doctor’s knowledge) and started her on amyotrophic lateral sclerosis herbal formula i ordered from Health Herbal Clinic, her symptoms totally declined over a 5 weeks use of the ALS disease natural herbal formula. She’s now almost 76 and doing very well, the disease is totally reversed!! Visit there website www. healthherbalclinic. net
I did the gluten elimination after having IBS symptoms all my life and after being seen by a gastro doctor and him telling me to eat plain pasta and crackers and bread. Of course I got worse when I followed his instructions and was much better after I did my elimination. I have problems with lots of other gassy vegetables, beans and legumes.